

Bad News and Some Further Neurogastro Stuff
First of all, some bad news that I will compress and explain as rationally as possible. I received the results of the neurogastro tests . Unfortunately, the neuropathological evaluation of the full thickness resection shows a (congenital)* myenteric hypoganglionosis/dyganglionosis/in segments an aganlionosis and also a ganglionitis. My enteric nervous system (ENS) ‘shows an unusually severe and rare finding with a manifold damage of the enteric nervous system which affects the ganglia cells and also the innervation’ which then manifests as a severe motility disorder that clinically manifests itself as intestinal pseudo-obstruction (IPO).
- Hypoganglionosis: Decreased number of nerve cells in the ENS of the intestinal wall (especially in the myenteric plexus) which clinically manifests as motility disorders such as Gastroparesis (stomach), slow transit constipation (colon), CIPO/enteric dysmotility (small intestine), achalasia (esophagus)
- Aganglionosis: Complete lack or loss of nerve cells (most famous form is the aganglionosis only inside the rectum = Morbus Hirschsprung)
- Dysganglionosis: pathological changes in the ENS e.g. immature ganglia cells (sometimes it is also an umbrella term for hypoganglionosis, intestinal neuronal dysplasia,…)
- (myenteric) ganglionitis: inflammation of the ganglions
which can affect segments or all of the large and/or small intestine, stomach, rectum and/or esophagus. For me, the whole GI tract from the duodenum up and including the rectum is affected. There are segments where the nerve cells are severely reduced or are completely lacking, those that are still there don’t show proper activity potentials and/or are in different states of dying (apoptosis***). Hence, we all know where this is going to lead to. I will sum up all my findings regarding neuropathology reports in the next few weeks (some kind of translation for others that are interested or want to understand their neuropathology report).
 So, please, don’t tell me that God will lead the way or that I will somehow find a solution with my mindset or that I will manage it just like I have overcome the struggles in the past years… I know that those conditions aren’t easy to understand for everyone, but you don’t tell someone with irreversible paralysis that they will be able to walk again.
So, please, don’t tell me that God will lead the way or that I will somehow find a solution with my mindset or that I will manage it just like I have overcome the struggles in the past years… I know that those conditions aren’t easy to understand for everyone, but you don’t tell someone with irreversible paralysis that they will be able to walk again.
Now, those conditions can be congenital (i.e. born with it, not necessarily genetic) or acquired*. Treatment options – if there exist any – differ here and also depend on the severity of nerve loss and nerve damage. For a congenital hypoganglionosis, for example, the number and the size of ganglia cells are both small at birth; their size does increase, but not the number of cells and dysmotility is programmed for life. Patients that suffer from an acquired hypoganglionosis are characterised by degenerating ganglia cells at some point in life. If there are certain segments that are affected and show severe dysmotility or atony (e.g. aganglionosis in the rectum aka Morbus Hirschsprung), those segments can be removed during a surgery (and a possible colostomy or ileostomy is inserted in the small or large intestine, respectively).
Further, the small intestine manometry showed a severe enteric neuropathy with no phase 3, no response postprandial, clustered bursts etc. As I have already explained earlier, you definitely don’t want an affected small intestine. The doctors advise against a colectomy (+ileostomy) since this wouldn’t solve the issue in the small intestine and would even trigger those pseudo-obstructions. Nonetheless, we might try a temporary loop ileostomy to basically simulate a colectomy.
- In an ileostomy an opening (‘stoma’) from the small intestine through the abdominal wall is created. The products that are normally transported further to the large intestine are collected in a bag. It can be temporary (i.e. removable, also called loop ileostomy) e.g. after surgeries for the affected intestine to give it time to heal i.e. the rest of the intestine is still kept and a permanent ileostomy e.g. after the removal of parts of the intestine (the large intestine is often removed in colonic inertia, certain cancer types or chronic inflammatory bowel diseases). In severe dysmotility those ileostomies can be used for venting.
- A colostomy is the same, but in the large intestine which can also be permanent or temporary. For dysmotility, there is also a caecostomy tube which makes irrigation possible, when the colon is affected and enemas aren’t possible anymore.
I am not doing well, we need another emptying/decompression via endoscopy and the symptoms are getting worse up to a continuous subileus state. Something needs to happen. So finger crossed for next week. I will have consultations with neurogastro, human genetics, neuropathology and a second opinion from another experienced gastroenterologist. Following the opinions of specialists in dysmotilities such as hypoganglionosis we need to do some more testings and depending on that we might find some kind of ‘therapy’ that can reduce symptoms – including the continuous and steadily increasing risk of an ileus and bowel perforation, sepsis, other organ struggles and a basically programmed end I do not want to explicate – even a tiny bit. Due to the progressive development and lack of other options I guess that I will get a PEJ/J Button quite soon and I do hope that it will reduce symptoms, especially regarding decompression and the duodenum could then dance all day and night without interrupting me, a bit. I won’t be off TPN anymore, but I would like to at least try enteral feeding via a PEJ as well.
- A PEJ (percutaneous endoscopic jejunostomy) is a tube that leads into the jejunum (small intestine) through the abdominal wall. It can be used for feeding, where it bypasses the stomach and part of the small intestine, and application of meds. In dysmotility it can be used for decompression, but the risk of dislodgement is high. It can either be placed in a lap surgery, x-ray guided or during endoscopy. After a month it can be swapped with a J Button for long-term usage. This one sits flat on the surface skin and you can then connect different extensions to it. For small intestine dysmotility one can use it for feeds, meds and irrigation in and venting out.
I will add a list of tube systems on the dysmotility site soon.
Vom Regen in die Traufe
Further, I desperately need a clinic or inter- and multidisciplinary team that accompanies my treatment which I do not have.
Of course, a patient should always cooperate and understand what’s going on (in the end, the patient can communicate symptoms far better – I do wait for the invention of a machinery that makes it possible for the doctor to feel what the patient is feeling), but a patient shouldn’t be his own doctor. Due to the accumulation of complex and rare (pre-existing and post-op(s)) I do not have a single doctor that is aware of my ‘patient history’, conditions and their interactions. I can be very lucky that I am
- A curious scientist at heart
- A former runner with a lot of endurance and energy
- A rebel who does not accept things that haven’t been completely proven
- Good at understanding complex relations and problem solving
- A tough cookie who has steadily reduced any expectations
I am afraid of the time I cannot rely on those anymore. I depend on the medical world. I need someone, some team out there that does not classify ‘my case’ as too complex or unique or closed and is willing to evaluate the full picture with all its nasty difficulties. I am sorry that I am a difficult, untreatable, expensive, fragile patient where normal protocols cannot be followed. I truly am.
But I am human also.

How do I react to bad news you cannot escape from, you cannot ignore or change? Bad news that is so difficult to accept and even let the slightest hopes evaporate? Too overwhelmed to think clearly? (and this doesn’t happen often with me) Worried. Sad. Disappointed. Angry. Lost. Helpless. Alone.
How to deal with bad news
- Think first. Don’t reply with immediate reactions. Don’t make a bad situation even worse.
- Switch off. What helps me most is switching off everything. Meditation. Nonetheless, don’t avoid them forever.
- Either: Think about the rational side only. What information did you receive, how will it affect you? Obviously, one can never put aside all emotions. Or: Let out all of your emotions. Cry, shout, sit in silence, be alone or be hugged by your loved ones… – it depends. In any case, accept your emotions (finally) and do not avoid them!
- See the positive in the bad news, as little as it might be, grow it and let its light outshine the major darkness. Reflect and reframe.
- Deep breathing. That’s something you can control at least.
- Ask for support if needed.
- Beware your body and mind balance, especially when the bad news concern your health.
More tips here.
Back then in the university clinic that stabilised me after I had been massacred in the hospital where the first surgeries were conducted, one doctor summed it up perfectly: ‘vom Regen in die Traufe’. We know what has followed after that and I wonder what will come next… A never ending storm flood. This basically means to swap something bad in favour of something else which is even worse… and that’s how my story has been developing the past years.
Traufe is the thing at the roof where rain collects/flows through before reaching the ground. Meaning, if you want to get protection from the rain under a roof, you might get even wetter when you are standing below the eave which I am sure everyone has experienced at some point. I’d prefer the rain. In the English language it is equivalent to ‘jumping out of the frying pan into the fire’ which is probably not that poetic (for once).
Anyway, it is even worse now. If the rain stops, you will be safe – also below the eave. But now we are experiencing a never ending rain (which now has even been forecast to only get heavier and heavier) and all I can do is swimming and swimming. With more difficulties comes less energy and swimming becomes more difficult, especially after several occasions of drowning. Nonetheless, somehow my body keeps moving upwards again. I don’t know where this magical energy comes from. As a physicist I know that it cannot come from nowhere. I am grateful for that.
Last week I watched the rain outside and thought – rain is beautiful, we know it will stop at some point. I was talking about nature’s rain.

Progress and goal making in chronic illness – planning for uncertain future
People that suffer from chronic conditions (life-limiting/threatening) also have the burden of a past, present and future with daily struggles and in between major unpredictable emergency situations. One day, a week, a few months, years…from needing more breaks, being immobile, long clinic stays to a bed-ridden daily life, it is impossible to have clear plans anymore.
Progress needs to be redefined in chronic illness. It does.
I have always been optimistic and ambitious (see below more on optimism). Before I got ill I always kept going. Running faster, running more, running unknown trails, extra projects here and there, activities, charities, projects. There were little times I took a break. Every day I improved. I improved my unicycle skills, my running, theatre playing, maths, physics, I helped out everywhere. Steady progress. Now I am fighting for survival.
How to accept that there is no progress (?) in some chronic illness conditions, especially those that are degenerative (in white on black and symptom manifestations). I don’t know what tomorrow will bring, I don’t know how much longer my body will be able to keep things going or how long my mind will be able to fight the constant physical stress. But I know that things are getting worse in my body, I know that it is irreversible and I know how things will likely develop to certain states, what interventions we will decide to have or will be urgent, and I know what complications will arise then… I am very well aware of that. I know that this whole accumulation of (rare and complex) conditions is so unpredictable that things might get very worse within this very next second. How to accept that there is no progress outside of my patient life? The patient life that has been getting so intertwined with my life.
So what I do is to think in seconds. What will I do in the very next second? And I am grateful when at the last second I managed the pain or nausea or didn’t faint. Should I stop planning or concentrating on long-term aims, well aware of the impossibility to reach my expectations? Well aware that it would put me into devastation? I think in little tip toe steps. I don’t know what to advise here anymore. Just like it is a problem in physics, we have to keep an eye on large-scale and small-scale dynamics.
I had so many plans. I wanted to run the Pyrennees, climb on Kilimandscharo and participate in ultra marathons trail runs; I wanted to live an independent life as a theoretical physicist and I wanted (…) – I have to stop here.

Always have some sort of plan, a backup plan and a backup of your backup and (…). Further, dynamic and constant adjustments need to be multi-factorial, interdependent and interconnected. Behaviour, physical, emotional, social, cognitive, … facets of life need to undergo changes while still maintaining your opinions, meaning and aims about life – your identification.
Setting goals, no matter how small, is important. It gives your purpose, identification and it gives you hope. It should be within your limits meaning the limits your chronic conditions set (not you! This is a huge difference). Nonetheless, less expectations, less disappointment. Find new meaning in tasks you are able to do. Plan them wisely, often it is easier to break them down in many small steps. Don’t urge yourself and accept breaks and cuts. Always remember that there are things you cannot regulate and there are things you can create, develop and succeed at!

Now, as promised
Absurdism, Pollyanna, Doors and Stones (and other thoughts in between)
 Lately, I have been imagining what Camus and Kierkegaard would have advised. Although Camus was born 100 years later than Kierkegaard it seems as if they have talked to each other through their workings. Camus categorised the Danish philosopher’s leap of faith (Fear and Trembling) on the same level as the ‘philosophical suicide’ (The Myth of Sisyphus).
Lately, I have been imagining what Camus and Kierkegaard would have advised. Although Camus was born 100 years later than Kierkegaard it seems as if they have talked to each other through their workings. Camus categorised the Danish philosopher’s leap of faith (Fear and Trembling) on the same level as the ‘philosophical suicide’ (The Myth of Sisyphus).
Shall I accept the absurd or turn to a (quick) leap of faith? Indeed, Kierkegaard does suggest turning faith (in God (?)) to overcome the absurd (I can’t speak Danish, but ‘leap of faith’ wasn’t actually mentioned). Camus, however, sees this as a gutless act of prodigal intellectualism. In my opinion, there is no either/or. Kiekegaard wants us to risk developing the faith, he wants us to jump into it. But does faith begin where thinking ends?
Camus emphasises that after being aware of the absurdity of life we can have three options: suicide (or rather philosophical suicide), leap of faith or facing the absurd – latter he suggests. But whereas the former means we simply accept something that doesn’t convince us, but is easier to digest, the second option gives us the possibility to live with the incomprehensible. Camus points out that only knowing about the existence of things we cannot explain, yet, we know it, is impossible. Kierkegaard circumvents this issue by defining the absurd as a condition in reality that cannot be explained by ratio alone. The leap of (rather by or towards) faith closes the gap.
I am not religious, but I would call this faith our deep rooted natural intuition, our sense of basic trust (in German called ‘Urvertrauen’). That’s what has kept me alive in the past years. No matter how often I experience new difficulties to overcome including mistreatment and negligence, my strength is fueled by this Urvertrauen. It gives me the possibility to transform reality to a state I can accept. A basic trust in humanity, nature, our bodies and environment, ourselves and the people around us – in faith and trust themselves. In some sense, that’s what Kierkegaard talked about, a deep trust in something-
Rationally, we cannot decide or justify what to do, so we might just take the leap. There is no reason in faith anymore, that’s why he suggests the leap. For Camus this leap is the rejection of reason in the fight against absurdism. However, Kierkegaard might reply that we should accept that we have to enlarge reason by faith. Whether it is turning towards faith or revolt, following Kierkegaard or Camus respectively, those paths are much nearer to each other than one might think. Both improve our awareness and move us towards true awakening.
Projected onto living with a chronic illness Kierkegaard might have said that the patient wants to be healed and Camus finds the patient as a happy person nonetheless.
Next time we will add Nietzsche to the round of non-existentialist like existentialists .

Not far away from Urvertrauen we find optimism. If one doesn’t know me properly one might think I am Pollyanna (‘an excessively cheerful or optimistic person’)**. Indeed, overly optimistic should probably be added on my pages-long diagnoses list.
It is understandable that people around me and doctors often misjudge this and miscommunication/understanding follows. On the other hand, I am pretty certain that otherwise I wouldn’t have made it through. It can’t be that bad, can it? My mum often asks me how I am able to keep my positive mindset. I wouldn’t actually define myself as a typical optimist, I have a realistic view of the future (meaning that there is none as it is simply unpredictable), but my reaction towards the situation in the past years might be unconventional to others. I would rather call it a state of awareness, mentally strong and strong- willed. I believe in myself and concentrate on the possibilities that are still left. And here I don’t distinguish between the unlikeliness or difficulties as long as it is still possible. A positive mindset is something we develop and have to use and care about every day.
Body and mind work hand in hand, so your mind set will definitely help during the adaptation to new normal life. I know others that are definitely doing better because of their optimistic and hopeful state of mind and there are countless studies that prove how important positive thinking for an improved feeling of health is. Nonetheless, this isn’t always and every time possible. The relationship with your (chronically ill) body is like any other relationship, there are good and bad times. External and internal factors can affect it. I call this relationship health. The only difference is that you won’t be able to have a break from each other (I won’t go into detail of the question what ‘you’ or ‘self’ actually is). Optimism probably increases activism, taking chances and using burdens as opportunities.
Yet, there have not been many studies whether unrealistic/naive optimism has the potential to damage rather than help. Here one should differ between thoughts and actions obviously… Health and illness aren’t opposites. If you are grateful for the health you have, you will enjoy life again.
Sometimes it is better to ‘disconnect’ from the body, sometimes to connect. You both have to decide and cooperate.




Look into all directions and adjust if needed. McLandburgh Wilson (1915) and/or Oscar Wilde described it very well:
Hence, keep your eyes on the donut. Maybe you are inside it and need to climb up to run around in circles to finally fly above it.
I might call a pragmatic optimism arisen by a strong will and need for improvement and innovation. Sometimes I also use it as a shield to protect myself from the hard truth. Or a realistic optimist and optimistic realist. And sometimes the only thing left is positive thinking. Positive thinking doesn’t assume anything, it is a choice I make about my response to the current situation.
A few notes on related topics can be found here, here and here. Optimism is also hope based on empirical facts. It becomes difficult if evidence based data is not available for the situation anymore tho.

Living. Living with uncertainty. Brings us closer to humanity. More choices and voices. More responsibilities and possibilities. More seriousness and experiences. Urvertrauen. Loss of control and the whole. Loss of predictivity and safety. Petrichor
Urvertrauen. What if you can’t trust (in) nature anymore? What if you can’t trust (in) your body anymore? Uncertainty. Absurdity. Emergency. Suffering. Uncomfortable. Recovering. Insufferable. Connecting. Accepting. Urvertrauen. Aufbauen. Isolation. Loneliness. Silent suffering. Stress. Disability. Invisibility. Vulnerability. Unpredictability. Complexity. Lack of empathy.
Waiting Fainting. Own disclosure. Grounding. Awaiting. What am I waiting for? What are you all waiting for? Is it easier to forget or to forgive? Regret. Relive. Upset. Prison inside me. Prison around me. Recover. Discover life. Floating. Drifting. Shifting. Aruption. Eruption. Interruption. Light in darkness.

More thoughts in between.
I repeat, health and illness aren’t opposites. If you are grateful for the health you have, you will enjoy life again. Even if there seems to be nothing left.
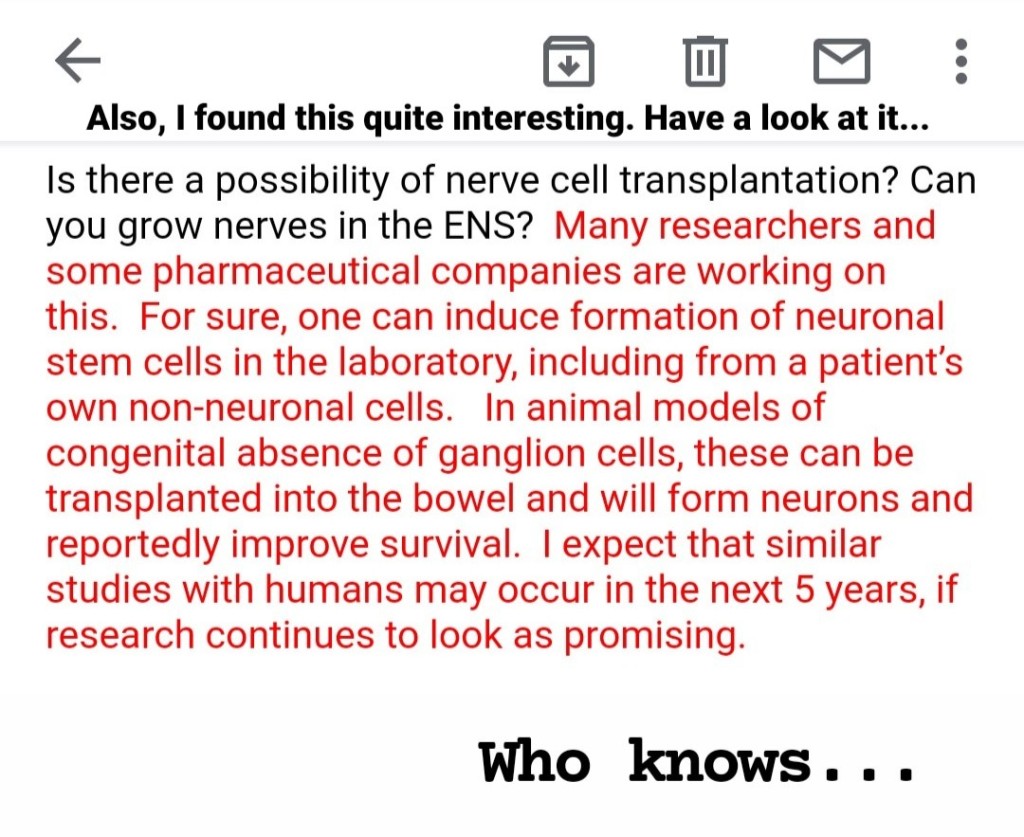
There was one sketch I recently came across that describes it quite well. Two doors, one just shut and the other opened with signs ‘shit’, ‘other shit’ – quite literally in my case. Bell gave that quote as well (without the shit). He also had to cope with many failures at first, but still continued trying. That’s what research is living for/of, right? Medicine is progressing, nowadays, there are available treatments one would never have thought about a couple of years back. In fact, I wondered whether there is a possibility to ‘grow’ nerves in the ENS for patients like me (intestinal failure due to nerve loss/dying nerves; Morbus Hirschsprung etc) and got a promising reply from a leading neurogastroenterologist. Here is a study of some transplantation in the colon of a mouse with slow transit. They use Enteric neural stem cells (ENSC) as source for potential new cells for the damaged ENS.
Indeed, when one door closes another door opens. However, often we waste our time by desperately trying to open that door or by staring at it full of regret and despair. We don’t realise the other door(s).
That’s exactly how chronic illness feels like. I could endlessly stare at the door that leads to a world of a physics career, ultra marathons, world travels, London night adventures and so much more. But it is closed. It was closed and it is impossible to open it… And whilst I am writing this I don’t agree with it. There is still some hope that it will magically open one day.
As we have seen, progress can/has to be redefined.
But even if I do realise the newly opened door, shall I step into it? Or shall I wait for another door to open yet again? How many doors have shut down during the time I am still concentrating on the other? Now, listen to ‘When One Door Opens’ by Joe Bonamassa… (also possible James Bond 2022+ theme)

How to deal with that?
- Be open and talk to your friends and family.
- Ask for help or whether they can visit you such that you are comfortable.
- Explain your condition.
- Start online/virtual meetings.
- Join support groups.
- Be brave to go out when you can.
- Try something new such as swap sports that you used to do with some light yoga. Learn something new, something you enjoy or inspires you e.g. learn a new language, knitting or cooking.
- Pets can change the world.
- Accept help via professional services (psychology appointments, call helplines etc).
- Help others out. Do something nice for your loved ones. That makes everyone happy and also takes away the thoughts on your current problems.
- Raise awareness.
- Make sure to know the difference between feeling a bit isolated or alone and depression. If you feel that you have serious problems talk with a doctor.
- Use your alone and isolated time wisely and try to enjoy it, use it as a time to become aware and recharge your body and mind. Loneliness and isolation can be positive as well.
More tips for things and stuff can be found here.
By the way, it is astonishing how things were adapted and made possible in the past year. Whether it is possible to work from home or speed up bureaucracy processes – when in the past and still today, people with chronic illnesses have lost their jobs and social life and/or haven’t had access to meds/medical equipment they need. It is astonishing to see how appointments in person can be done virtually nowadays. It is astonishing how people complain about the quarantine and ‘loss of life’ when there are people out there that have been living in quarantine for years or decades! Patients have literally lost a whole year due to the pandemic. Treatments, surgeries, diagnostics (…) were stopped.
I hope that the global pandemic also helps in this sense. People have a reference now on how it is to live in isolation. For many it has been a long isolation and will continue to be, even after the pandemic. Moreover, physical isolation should be distinguished from emotional one, where the latter is often amplified by poor physical conditions.
Conditions can also change around you, they can be adapted and adjusted.

In Germany, we have the collocation ‘Steine in den Weg legen’ – place stones in the way (put unnecessary obstacles in the way). I like that we use the term ‘Steine’. Who says that those stones are obstacles? Stones can be used to build and create. Life is a rocky path.
One should follow the path available and we are convinced of and build our future with, around or/and on the obstacles we face. We should give our best to make something positive out of the difficulties we face.
We will grow with it. The more stones you have the more you can build, right?
Turn apparent obstacles into opportunities (recall, opportunities in the end are the ones that turn into obstacles… it is a constant flow!). It’s all about the perspective we choose to apply. Often we simply cannot change the obstacle, but we can change its reflection in our eyes. Let’s start today. What is an obstacle you are facing right now? Start with a minor one. Why do you feel that this is an obstacle? Try to reduce and be aware of your emotions. Now ask the following questions: Has this always been and will it always be an obstacle? What is the importance of it? Finally, think of at least one opportunity you can take from facing this obstacle. Be proud of and look forward to the future you will have mastered.

Isn’t that beautiful?
Think about the stone’s perspective:
Maybe in a river bank, safe at first, burning in the sun in the dry summer. Looking forward to the refreshing, cooling rain. Then inside of deep and wild rushing storm floods – slowly moving. Frozen in the winter. Standstill. Warming up and moving again. Animals. People come and go. Movement. In the stream, with the stream, out of the stream. Animals sniffing. People tell their sorrows and hopes. Maybe from the top of the mountain down to the rivers to finally reach the ocean. Probably exciting, but yet of such a firm existence at rest. Decades, centuries, millenia. Maybe witnessing the cyanobacteria, dinosaurs and mammoths, from the oceans and the lands. Silently observing. Changes. Ice ages and warm periods. Asleep. Climate crisis and humanity.
They have to accept their dependence on the environment. A passive life in constant reactions towards nature’s forces. Maybe from a big rock to a little pebble. Stable in the heaviest storms and taken away by a light summer breeze. From the Nuvvuagittuq Greenstone Belt to Birdlings Flat. Time becomes perception. Time perception.
A stone can be anything, it can be a whole world.

How many times must a man look up
Before he can see the sky?
Blowin’ in the Wind, Bob Dylan

All political interpretation aside, for me this song from 1963 is about how truth and enlightenment is all around us. We can feel it, sometimes more and sometimes less. Yet we cannot grab or see it. We cannot simply ignore it. The invisibility is facing us. The answers and changes to occur are floating around us, but we have to be willing to form them into thoughts, words and actions. We should blow in and with the wind, more freely. Circumventing (apparent) obstacles. Following pressure differences, nature, to equate and stabilise. In Japanese philosophy wind (‘fu’) stands for growth, development and movement in freedom. Just like the wind we should grow and learn, turn our knowledge, passions, skills and experiences into parts of the cosmic dance. Breathe openly and deep. With the wind blowing those answers are constantly changing and we have to accept to be part of this dynamic flow. We have to endure it, this is the price of being alive.
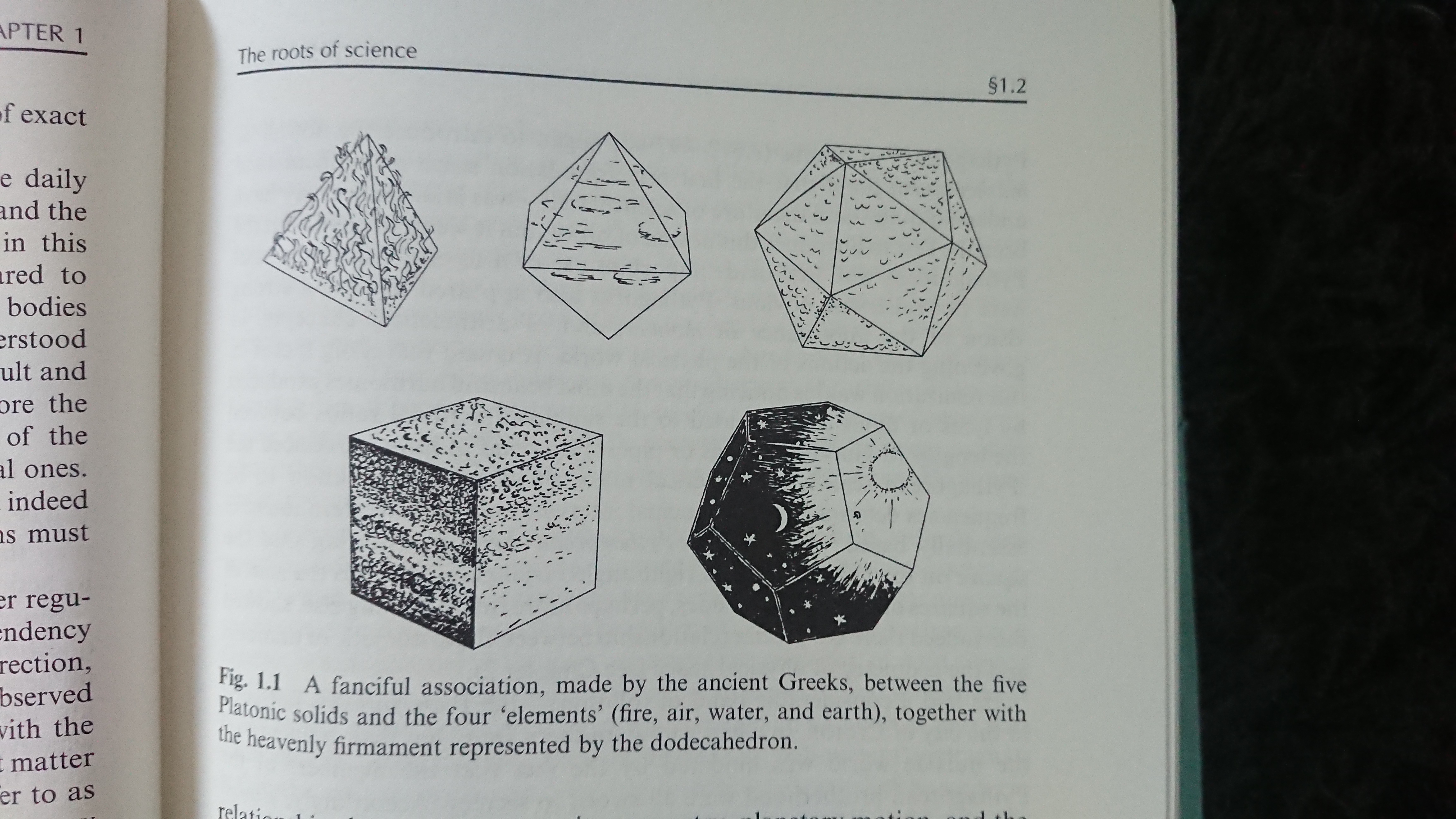
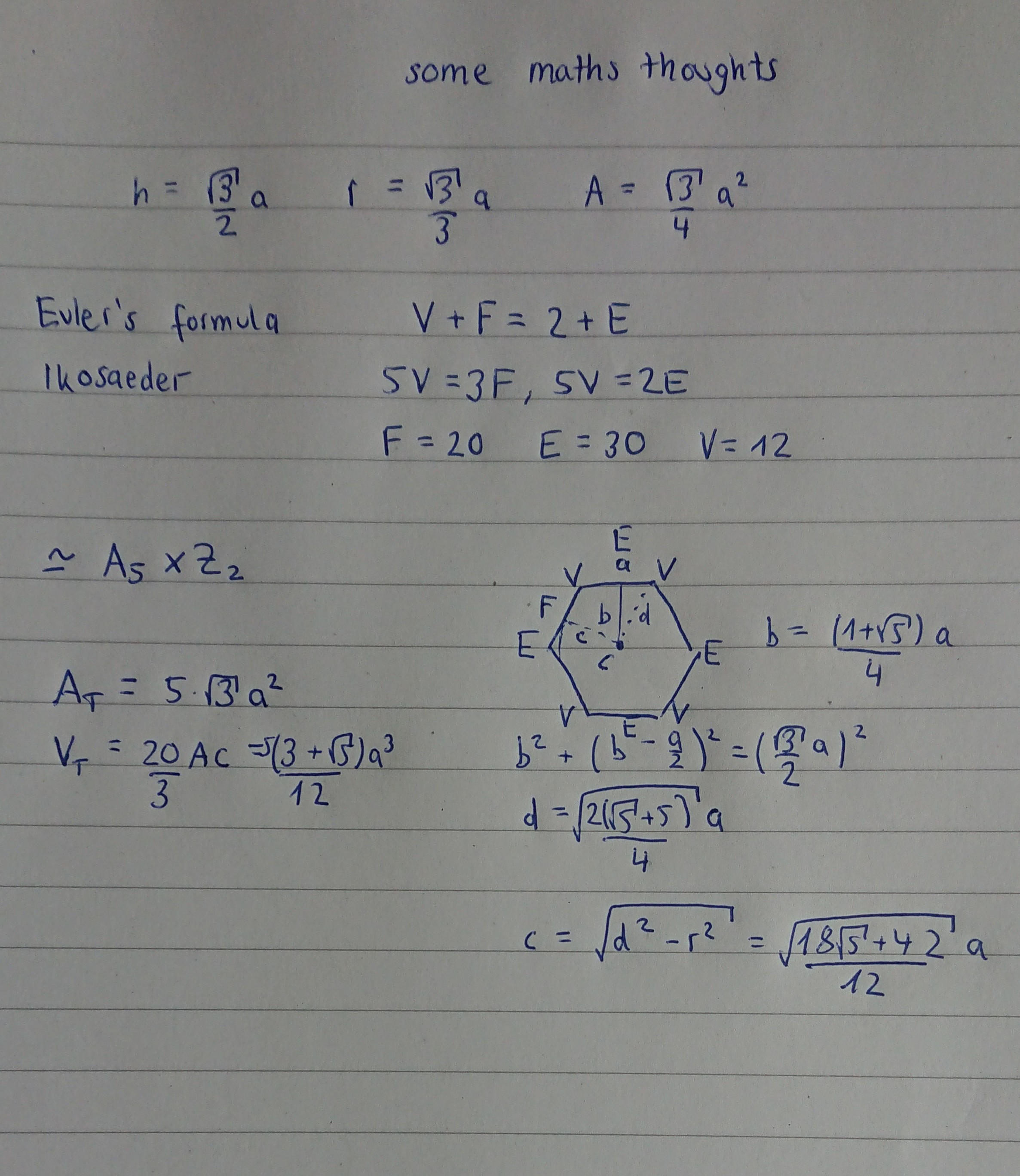
I am sure that Camus would have agreed. It also is a protest against naivety, injustice and its ignorance, a protest for courage, hope and peace. Wind is moving air. Air is the ikosaeder, the platonic body (see below, excerpt from ‘The Road to Reality’ by Penrose) where five triangle faces touch each other at each vertex. Here you have a quite astonishing manifestation of the golden ratio: Connect four vertices in a plane inside the ikosaeder to a rectangle, you will get three that cut according to the golden ratio. An ikosaeder has 20 faces and 12 vertices (i.e. 12 + 20 – 2 = 30 edges), for the dodekaeder it is the other way around (they are dual – if you connect the centres of the sides you will get the dodekaeder, if you connects their centres again you will get an ikosaeder again). Latter represents the spirit, the unanswered or left part that cannot be presented by the four elements of nature. It is the air that lifts our spirit embracing the air again. By the way, ikosaeder and dodekaeder united can give us wonderful objects, for example a football.
Further Recommendations and Tips
Sleep in, please body cooperate – songs
- Falling Into the Skies, Great Lake Swimmers (whole album: Bodies and minds)
- Still, Hayden Everett
- Swim, Hoe Hicks
- Disenchanted, My Chemical Romance
- Places We Won’t Work, Bruno Major (We will smile to end each day/ In places we won’t walk)
- Wait, M83 (Send your dreams where nobody hides/ Give your tears to the tide/ No time)
- Call It Dreaming, Iron & Wine
- From Eden, Hozier
- Shibari Moon, Oscar Key Sung
- Tin Lover, The Paper Kites (When the cold is over/ Pull me out the ground)
- Runaway, Aurora
- Childhood, Roo Panes (Everyday’s a childhood/ Everyday’s a wild wood)
- Blue Knuckles, Night Beds
- So Simpatico, Villagers
- The Astronaut, Wax Fang (whole album)
It’s so hard to breathe in here\ Can anybody please hear me out there?
…
Death from life\ Life from death\ Time does not exist\ Pain is our limit
…
Suddenly I have a feeling\ That I am no longer human\ I can’t tell where my skin ends
And the space around me, it begins\ No need to breathe\ No need to eat\ No need to sleep
The Astronaut

Think before you speak
But you don’t look sick. I always wonder, how does one look to be classified as sick? Only when I am hooked up, the moment I am vomiting or screaming in pain? The moment just before I faint? Only when I am on the ICU again?
You don’t look like… like what?
When are you getting better? You still don’t feel better? Are you feeling better yet? It seems that you are still not better. Lazy me!
What an interesting case you are. I have never come across a case like you. I am not a case or number, please.
You can be lucky that you are still alive. You look pretty well considering you almost died. That’s the most wonderful compliment I have ever received, thank you! And you look quite smart considering ...
Really? I don’t believe that. (…) *visual proof. evidence.* **no apology**
You look good with your red cheeks (butterfly face reacting to something again and feeling pretty bad).
Well, you are young, so I guess you don’t need any help when moving? *about to faint due to too much standing already*
Nah, I don’t believe those values. Let’s take another measurement. (…) Weird, are you OK?
We have never experienced this. We have never had such a problem or complication. *It must be your body.* **It is your fault.**
We don’t know how to proceed anymore. You should see specialist A. *recommends specialised specialist B who sends me to super-specialised super-specialist C* **no overview whatsoever anymore**
You shouldn’t be in so much pain. *You call this pain?*
Crazy, that’s really crazy. Wow. So is there a cure?
I know how you feel, I am also quite tired.
I also have that tummy ache every now and then.
Have you tried xxx? My friend’s friend has done it and it worked miracles.
So, how long have you been in the hospital? / Just a week. / Oh, poor you. *basically living in clinics.*
You are probably happy that you can go home now and you’ll be better. *Discharge doesn’t mean your condition has improved at all.*
Well, if you are still able to study it cannot be that bad.
It could be worse.
Just keep going.
I know exactly what you are going through.
Why are you always cancelling?
*simply ignoring the whole situation* or *talking about a totally unrealistic future*
I haven’t messaged, because I don’t know what to say. Thank you for the information.
Usually, I don’t react to such comments. I think I still laugh, because I want people to feel comfortable around me. Or I simply ignore it. Sometimes, however, I have to tell the truth. Always recall that there is so much you don’t see, you cannot assume or conclude. I don’t want people to see my/our struggles.
Often it is simply because of poor word choices when intentions are actually very different. Communication is the basis of every treatment whether between patient and doctor or between family members or friends.
There are studies that show that
- Attentive responses
- Support for self-reliance
- Acting as a whole
- Honest encouragement
Improve life quality of chronic illness sufferers. Whereas,
- Passive responses or distraction behaviour
- Controlling or criticising actions
- Overprotective behaviour
- Frustrating mindset
Made things worse. Obviously, communication is both ways such that it highly depends on us patients, too. Honesty and transparency are needed for assertive communication.
From my own experience I can say that neutral behaviour is the most effective. I don’t want to be asked every few minutes how I am doing or how people are sorry, but on the other hand I find total ignorance sometimes quite hurtful. Set your limits, on both sides. Next time I will go into detail of patient-doctor communication. Further tips for things and stuff can be found here.

Ask for Support songs – you are not alone:
- Ask For Help, Kings of Convenience
- Two/ Sylvia, an Introduction, The Antlers
- Just Be Held, Casting Crowns (So when you’re on your knees and answers seem so far away/ You’re not alone, stop holding on and just be held/ Your world’s not falling apart, it’s falling into place)
- Wish You Were Here, Milk Carton Kids
- Collapsed in Sunbeams, Arlo Parks (You’re not alone like you think you are/ We all have scars, I know it’s hard/ …/ With you I’m always making rainbows out of something painful/ Getting fried is how I’m dodging gravestones/ …)
- In Quiet Moments/ Every Beat That Passed, Lost Horizons (whole album) (Will we be the next ones to fall?/ Will we be the next ones to rise?)
- easier , Slenderbodies (whole album are we?)
- Good Day, Twenty One Pilots (Is a buzz and a light, I’ll be singing out/ I know it’s hard to believe me, it’s a good day)
- Long Lost, Lord Huron (I’ve got a place in the world/ And I found my way/ Out in the night all alone/ In the way out there/ I ain’t lonely/ I’m long lost)
- Convocations, Sufjan Stevens (see below)
Latter is basically humanity set to musical cycles. It covers meditations, lamentations, revelations, celebrations and incantations summing up to convocations. I guess he is known for his hard work, but that instrumental collection is crazy. It is his personal reaction to loss, how his emotions flowed and changed through those stages.
First we reflect what has happened, spotted by some moments of confusion and disorientation in meditation. We might anticipate what is coming next.
Lamentations follow. We are faced with the realistic, hurting and sad truth.
Revelations provide us with explosions, the discovery of acceptance. We are looking farther out than before.
We finally arrive in celebrations of life, celebrations of what was sparkled by moments of gratefulness. The whole has always light and beauty in it.
For me this is also a way of healing.
It ends with the incarnation, the resolution of prior tensions.
I particularly enjoyed the dimensional part of it.

Distraction and Encouragement recommendation
Since we might try the ileostomy and this is obviously something one needs to get along with, I came across the youtube channel of Garrett Taira. He has been suffering from Cipo as well and his way of dealing with the daily struggles, his gratefulness for his family and friends and the way he sees the positive in every situation, is very inspiring. Even if you don’t suffer from dysmotility, it is a fun channel to watch.



If you suffer from nausea attacks or pain at night or insomnia (for those in Europe), watch the final of Copa América (2am CEST).
Meanwhile, Einstein is practising for his Ninja career.

*I do not believe that it is congenital. I have been in contact with leading neurogastro and neuropathology specialists and worked through papers (which is quite difficult as those conditions are extremely rare if not individual which makes it difficult to compare) and we all agree that a congenital condition should have manifested far earlier. Plus, one shouldn’t forget that both, my ANS (via the first surgery) and the ENS, are damaged/dead. Further tests are needed and I will update soon. I believe that the hypoganglionosis is caused by a chronic myenteric ganglionitis and NOT the other way around. Hence, we need to find the cause for the ganglionitis which is dominated by CD8+ T-cells (if there is some expert out there reading my blog, please, I would be so grateful if you could point us in the right direction – also no B-cells, very weak immune response and CD163+ macrophages in the myenteric plexus). It could be post-viral infections, autoimmune-related processes … Those connections aren’t fully understood yet (some of which aren’t understood at all); so it is a huge task to find the needle in the haystack. I hope to talk with the neuropathology team next week, we could analyse the biopsy again as well as blood draws for specific antibodies. If there is any chance that it is autoimmune related we could try immunosuppressive therapies to prevent (at least) further cell death.
** taken from the children book Pollyanna where the little girl gets taught to be grateful for her birthday present of crutches that she doesn’t need. If you look close enough she doesn’t live a life of joy only, but her perspective towards difficulties makes it seem to be so. Now have a listen to Green Day’s Pollyanna.
***Interestingly, apoptosis originates from the Greek word which means ‘leaves falling from a tree’ which describes it quite poetically… Our ENS is a wonderful construct and the nerve cells have some kind of intrinsic programmed death just like we know that in Winter the trees will lose their leaves. Unfortunately, here they won’t grow again.

4 thoughts on “A Leap of What?”